Ending Unequal Treatment: Strategies to Achieve Equitable Health Care and Optimal Health for All (2024)
Chapter: 8 Accountability
8
Accountability
The evidence presented in the preceding chapters documents the significant advances in health care policy and practice since Unequal Treatment was published 20 years ago. The legal and regulatory environment is markedly different, as noted in Chapter 4, and many other changes have occurred. For example, positive changes in access to care have come from major expansions in health insurance coverage, improvements in electronic medical records and other mechanisms to gather data, improved knowledge about what works to improve outcomes and reduce inequities, and a better understanding of the role of the structural and social determinants of health and the capacity of systems to measure outcomes. In other areas, the changes have been negative, such as the loss of critical hospital infrastructure in rural communities and worsening provider shortages throughout the system. Amidst significant changes, inequities persist, and advancing toward an equitable health care system that contributes to achieving optimal health for all remains a desired goal and one of the drivers of this consensus study.
But the findings presented in this study also underscore just how far the nation has to go where health care equity is concerned, by documenting the extent to which, 2 decades after Unequal Treatment, racial and ethnic inequities remain throughout the health care system. Racially and ethnically minoritized populations disproportionately rely on forms of health insurance that pay noncompetitive rates and leave them more dependent on health coverage arrangements with narrower provider networks and more
access-limiting controls. The evidence also points to less robust treatment even among minoritized patients in the same health care systems as their White counterparts. The United States also has not promoted and deployed a diverse health and scientific workforce, reflective of the U.S. population and with the training, skills and knowledge needed to promote more equitable health care system performance.
Enduring, robust results demand a deep commitment to change systemwide, greater investment in the tools needed to make changes, ongoing research to document what is and is not working, and a willingness to change practices and behavior to more fully embrace what does work. As described in Chapter 4, the ACA was an important step forward in realizing many of the changes that Unequal Treatment contemplated. However, some of the ACA’s reforms were less than what was needed, and others have not been implemented adequately. Chapter 5 details how the U.S. health care delivery system has not fully embraced health equity’s value and imperative or systematically implemented promising changes. Chapter 6 outlines the central role of communities and the importance of community-based, community-partnered health care. Chapter 7 discusses how research can further support progress toward eliminating health care inequities and advancing health equity.
The committee recognizes that many initiatives to change how the health care system functions have not been successful despite multiple national reports with actionable and thoughtful recommendations for improvement, and efforts to advance racial and ethnic health care equity have not resulted in long-term gains. A limited number of the recommendations from Unequal Treatment have been fully implemented. A major challenge has been a lack of accountability and processes to support sustained and measurable progress.
Effective accountability requires focus and attention across a broad range of areas and actors. For example, from a federal law and policy standpoint, accountability begins with Congress and its legislative response to the social problems affecting health care and health equity. Legislative oversight needs to ensure that laws have their intended impact and identify actions needed to improve their performance. This often requires federal agencies to create and enforce policies. Within the health care system, public and private actors are subject to laws and standards. Accountability helps to ensure compliance and constant measurement to evaluate challenges and areas of success. For private actors, accountability also entails self-regulation through standards of accreditation and measures of self-governance.
Guided by the committee’s conceptual framework (see Chapter 1), this chapter outlines current accountability structures and processes and
discusses what is not currently working and what is needed to hold society and actors accountable for accomplishing health care equity goals. As discussed throughout the report, the committee recognizes that health and health care are different but inextricably linked. Health is a state of complete physical, mental, and social well-being and not merely the absence of disease or infirmity, while health care refers to the services provided to individuals, families, and communities for the purpose of promoting, maintaining, or restoring health across settings of care. Furthermore, the committee acknowledges that reductions in health inequities will require simultaneous improvements to health care as well as the many factors beyond health care that influence health. Therefore, this report uses “health care system” (activities related to the delivery of care across the continuum of care) to describe the U.S. health care system as a whole and individual health care systems and “health” when discussing outcomes.
ACCOUNTABILITY STRUCTURES AND PROCESSES
Creating systems of accountability to ensure that laws and policies have their intended impact to achieve health care equity and optimal health for all without unintended consequences is a major challenge in the United States. Accountability requires leaders, actors, and entities at a variety of levels to accept responsibility for the health of the individuals and populations they serve.
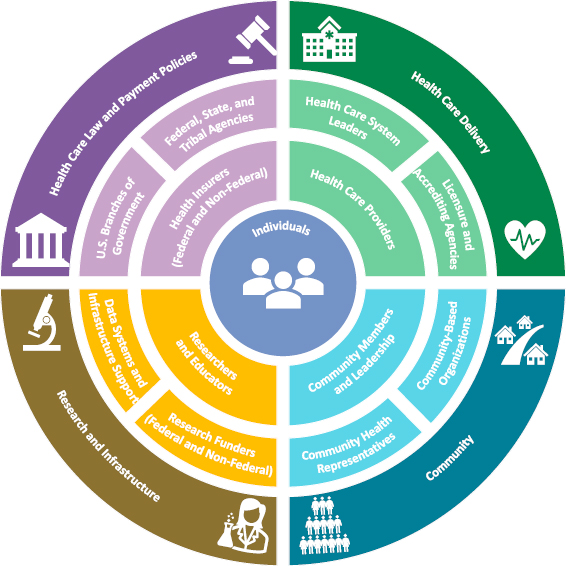
Accountability is intertwined with all other domains that need to work together effectively to achieve an equitable health care system. As an example, data and research are essential resources for achieving effective implementation, enforcement, and compliance. Accountability structures and processes, in terms of health care laws and payment policies (Chapter 4); health care delivery (Chapter 5); community centeredness and engagement (Chapter 6); and research findings, data, and infrastructure (Chapter 7), are dynamic, complex, and interactive. The next sections present an overview of the key places in the health care system where accountability is needed and the actors accountable for accomplishing health care equity goals. Guided by the committee’s conceptual framework in Chapter 1 and the discussions in the prior chapters, Figure 8-1 is a visual representation of these key places and the major actors accountable.
Blumenthal and colleagues (2021) have described a potential framework by which the Center for Medicare and Medicaid Innovation can make health care systems accountable It defines levers for accountability, such
as data and measurement, payment, public reporting, accreditation, and regulation; and holding actors (e.g., clinicians, hospitals, health plans, suppliers, government agencies) accountable for achieving optimal outcomes in broad areas, such as quality, cost, and equity (see Table 8-1). Such a framework could be advanced to hold the broader part of the health care system accountable.
HEALTH CARE LAWS AND PAYMENT POLICIES
Legal and Policy
The Agency for Healthcare Research and Quality has published the National Healthcare Quality and Disparities Report to highlight trends across health care settings over the past 2 decades. Federal, tribal, state, territorial, and local governments have made efforts to hold themselves and other actors accountable for reducing racial and ethnic health and health care inequities. For example, the federal government uses several
| Levers for Accountability | Actors to Hold Accountable | Outcomes |
|---|---|---|
| Payment: applying upside and/or downside financial risk through retrospective or prospective payments (e.g., bundled payments, accountable care organizations) | Health Care Providers: provider groups, practices, hospitals, integrated health systems | Quality: improving quality and safety of care, including patient experiences |
| Measurement: tracking performance on specific outcome metrics over time or cross-sectionally (e.g., HEDIS, CAHPS) | Health Plans: Medicaid managed care plans, Medicare Advantage plans, commercial plans | Equity: reducing disparities by race/ethnicity, gender, income, geography, social risk, etc. |
| Public Reporting: making performance data public (e.g., Medicare Compare, star ratings) | Geographies: states, metropolitan statistical areas1 | Cost: lowering costs or ensuring cost-neutrality of care |
| Accreditation: requiring certain behaviors or actions to be certified as safe and of sufficient quality (e.g., Joint Commission), often required for participation in Medicare or Medicaid programs | Suppliers: durable medical equipment, pharmaceutical industry, IT vendors | |
| Regulation: applying standards through federal regulation (e.g., risk adjustment, network adequacy) | Government Agencies: Centers for Medicare & Medicaid Services | |
| Consumers: patients, health care providers, family, community members |
SOURCE: Blumenthal et al., 2021.
___________________
1 A geographic entity based on a county or a group of counties with at least one urbanized area with a population of at least 50,000 and adjacent counties with economic ties to the central area. See https://www.cdc.gov/nchs/hus/sources-definitions/msa.htm (accessed April 29, 2024).
BOX 8-1
Select Recent Executive Orders to Advance Health Equity
Executive Order 14091: Further Advancing Racial Equity and Support for Underserved Communities Through the Federal Government (2023): To continue to advance racial equity and support for underserved communities through the federal government by extending and strengthening equity-advancing requirements for agencies and positioning them to deliver better outcomes for the American people.
Executive Order 14110: Safe, Secure, and Trustworthy Development and Use of Artificial Intelligence (2023): To advance and govern the development and use of artificial intelligence (AI) in a safe, secure, and responsible manner, while promoting innovation, competition, and collaboration. The order also emphasizes the importance of addressing health equity and civil rights, as it aims to ensure that AI systems comply with all federal laws and promote robust technical evaluations, careful oversight, engagement with affected communities, and rigorous regulation to protect against unlawful discrimination and abuse.
Executive Order 14035: Diversity, Equity, Inclusion, and Accessibility in the Federal Workforce (2022): To strengthen the federal workforce by promoting diversity, equity, inclusion, and accessibility (DEIA), as it establishes a government-wide initiative and strategic plan to advance these priorities across the federal workforce.
Executive Order 14075: Advancing Equality for Lesbian, Gay, Bisexual, Transgender, Queer, and Intersex Individuals (2022): To
mechanisms including executive orders, congressional actions, and federal agency initiatives. Recent executive orders have aimed to strengthen equity throughout government, including areas in the health care sphere where the federal government has the greatest influence (e.g., access to health care, payment of services, and health care professional training) (see Box 8-1). In addition, bills have been introduced in Congress related to health care equity (see Box 8-2). However, many of these draft bills have not been translated into laws and concrete policies.
Several Department of Health and Human Services (HHS) agencies have developed frameworks or published strategic plans to further
advance equality for lesbian, gay, bisexual, transgender, queer, and intersex (LGBTQI+) individuals by addressing systemic discrimination and barriers they face in various aspects of life, including health care.
Executive Order 14009: Strengthening Medicaid and the Affordable Care Act (2021): To strengthen Medicaid and the Affordable Care Act (ACA) by making high-quality health care accessible and affordable for everyone in the United States. The order addresses health inequities by establishing a Special Enrollment Period for uninsured and underinsured Americans to seek coverage through the Federally Facilitated Marketplace, as well as reviewing and potentially revising or rescinding agency actions that may undermine protections for people with preexisting conditions, reduce coverage under Medicaid or the ACA, or present barriers to accessing health care coverage.
Executive Order 13985: Advancing Racial Equity and Support for Underserved Communities Through the Federal Government (2021): To advance racial equity and support for underserved communities through the federal government by addressing systemic barriers and promoting equal access to opportunities and benefits.
Executive Order 13166: Improving Access to Services for Persons with Limited English Proficiency (2022): To renew the federal government’s commitment to its language access obligations. The order requires federal agencies to examine the services it provides and to develop and implement a system by which people with limited English proficiency (LEP) can meaningfully access those services consistent with, and without unduly burdening, the fundamental mission of the agency.
understand and address the persistent racial and ethnic inequities in health care (see Table 8-2). However, these plans are often siloed and disconnected, with no unified oversight or evaluation of programs or policies.
The many proposed federal policies and executive orders illustrate a strong national commitment to advancing health equity. However, few of these policies are effectively enforced, which speaks to the challenges of accountability within the federal government. The HHS Office of Civil Rights (OCR) enforces policies that promote health equity. As mentioned in Chapter 4, OCR is responsible for enforcing accountability by addressing
BOX 8-2
Select Draft Bills Related to Health Care Equity
S.3073 - Equal Health Care for All Act of 2021: This bill would prohibit discrimination in health care based on race, religion, and other characteristics. It also revises reporting requirements, adds equity-related measures to certain Medicare programs, and makes other changes to reduce care inequities.
S.4486 - Health Equity and Accountability Act of 2022: This bill would direct HHS and other agencies to undertake efforts to reduce health disparities.
S.1219 - Health Equity for People with Disabilities Act of 2023: This bill would modify certain grants available to health centers that offer primary health services to medically underserved populations to ensure that members of such populations with disabilities receive accessible health services.
H.R.5742 - Equitable Health Care for All Act of 2021: This bill would prohibit discrimination in health care based on race, religion, and other characteristics. It would also revise reporting requirements, add equity-related measures to certain Medicare programs, and make other changes to reduce health disparities.
H.R.1029 - Territories Health Equity Act of 2023: This bill would alter provisions relating to the treatment of U.S. territories under Medicaid, Medicare, and Medicare Advantage. For example, the bill would eliminate Medicaid funding limitations for U.S. territories; exempt an individual from late-enrollment penalties for Medicare medical services if the individual resided in Puerto Rico as of the date of eligibility and the individual enrolls within 5 years of such date; and establish minimum criteria for certain elements used in Medicare Advantage payment calculations for areas within U.S. territories.
H.R.3548 - Pursuing Equity in Mental Health Act of 2023: This bill would address mental health issues for youth, particularly youth of color, and authorize funding to support research, improve the numbers of culturally competent providers, build outreach programs that reduce stigma, and develop a training program for providers to effectively manage inequities.
H.R.4585 - Advancing Maternal Health Equity Under Medicaid Act of 2023: This bill would amend title XIX of the Social Security Act to provide a higher federal matching rate for increased expenditures under Medicaid for maternal health care services.
H.R.3305 - Black Maternal Health Momnibus Act of 2023: This bill would target ending preventable maternal mortality, severe maternal morbidity, and maternal health disparities in the U.S., and invest in addressing adverse social determinants of health that influence maternal health outcomes.
| Document Type | Agency | Report Title (Date) | Brief Summary of Document |
|---|---|---|---|
| Action Plan | Department of Health and Human Services (HHS) | HHS Equity Action Plan (2022)2 | This plan describes actions HHS can take to advance health equity and institutionalize a focus on it, highlighting five key HHS activities as examples. It focuses on advancing equity in the delivery of health and human services as part of the presidential administration’s broader efforts to promote equity. |
| Action Plan | Centers for Medicare & Medicaid Services (CMS) | CMS Outlines Strategy to Advance Health Equity (2023)3 | This plan includes a comprehensive approach involving all CMS centers and offices, focusing on closing health care gaps for underserved populations and promoting culturally appropriate services. |
| Action Plan | Department of Veterans Affairs | Health Equity Action Plan (2024)4 | This plan is aimed at reducing health disparities among veterans and ensuring equitable health outcomes. It encompasses addressing disparities across various demographic groups, such as race, ethnicity, gender, age, and disability. It emphasizes increasing awareness, strengthening leadership, improving health outcomes, enhancing workforce cultural competency, and advancing data collection and evaluation methods. |
| Policy Document | CMS | CMS Physician Payment Rule Advances Health Equity (2024)5 | This rule proposes coding and payment for several new services to help underserved populations. It includes provisions for caregiver training, community health integration services, Principal Illness Navigation services, and social determinants of health risk assessments. It aims to improve access to behavioral health in Medicare and proposes increased payment for crisis care, substance use disorder treatment, and psychotherapy. |
___________________
2 See https://www.hhs.gov/sites/default/files/hhs-equity-action-plan.pdf (accessed April 29, 2024).
3 See https://www.cms.gov/files/document/cms-strategic-framework-fact-sheet.pdf (accessed April 29, 2024).
4 See https://department.va.gov/wp-content/uploads/2024/02/Department-of-VeteransAffairs-Equity-Action-Plan.pdf (accessed April 29, 2024).
5 See https://www.cms.gov/newsroom/press-releases/cms-physician-payment-rule-advances-health-equity (accessed April 29, 2024).
| Document Type | Agency | Report Title (Date) | Brief Summary of Document |
|---|---|---|---|
| Policy Document | CMS | CMS Proposes Policies to Advance Health Equity and Maternal Health, Support Hospitals (2024)6 | This policy focuses on addressing health care disparities in hospital inpatient care. It proposes three health-equity-focused measures for the Hospital Inpatient Quality Reporting Program. The measures assess a hospital’s commitment to establishing a culture of equity and include screening and identification of patient-level, health-related social needs. |
| Report | Agency for Healthcare Research and Quality (AHRQ) | 2023 National Healthcare Quality and Disparities Report (2023)7 | AHRQ presents trends for measures related to access to care, affordable care, care coordination, effective treatment, healthy living, patient safety, and person-centered care. |
| Report | Substance Abuse and Mental Health Services Administration (SAMHSA) | Approaches in Implementing the Mental Health Parity and Addiction Equity Act: Best Practices from the States (2016)8 | This report offers best practices for implementing the Mental Health Parity and Addiction Equity Act of 2008. It covers processes for implementing parity and collaborating with other organizations and also tools for understanding and monitoring compliance. |
| Report | CMS | CMS Framework for Health Equity 2022-2032 (2022)9 | This report presents a decade-long pathway to advance health equity and expand coverage within Medicare and Medicaid. |
| Report | Centers for Disease Control and Prevention (CDC) | CDC Global Health Equity Strategy 2022 – 2027 (2022)10 | This report details an agency-wide health equity science and intervention strategy to holistically reimagine how CDC approaches health equity. |
___________________
6 See https://www.cms.gov/newsroom/press-releases/cms-proposes-policies-advance-health-equity-and-maternal-health-support-hospitals (accessed April 29, 2024).
7 See https://www.ahrq.gov/research/findings/nhqrdr/nhqdr23/index.html (accessed April 29, 2024).
8 See https://store.samhsa.gov/sites/default/files/sma16-4983.pdf (accessed April 29, 2024).
9 See https://www.cms.gov/files/document/cms-framework-health-equity.pdf (accessed April 29, 2024).
10 See https://www.cdc.gov/globalhealth/resources/reports/annual/22/equity.html (accessed April 29, 2024).
| Document Type | Agency | Report Title (Date) | Brief Summary of Document |
|---|---|---|---|
| Strategic Plan | CDC | CDC Office of Health Equity’s Work in Advancing Health Equity (Ongoing)11 | This initiative encompasses various efforts, such as Project Firstline for health care workers’ infection control and global programs to improve the health of girls. It focuses on advancing health equity through education, resource provision, and addressing cultural and gender-based discrimination. |
| Strategic Plan | National Institutes of Health (NIH) | NIH Strategic Plan (2023)12 | This plan covers fiscal years 2023–2027 and demonstrates NIH’s commitment to integrating diversity, equity, inclusion, and accessibility (DEIA) principles across all its activities. It focuses on enhancing DEIA in operations, workforce, and research, aiming to achieve better health for all. The plan outlines goals and strategies in these key areas and includes approaches to advance DEIA both within NIH and in the broader biomedical and behavioral research enterprise. |
| Strategic Plan | NIH | NIH Minority Health and Health Disparities Strategic Plan 2021-2025 (2023)13 | This strategic plan charts the path for NIH to advance the science of minority health and health disparities. It lays out a comprehensive strategy for the next 5 years and beyond, encompassing scientific goals, research strategies, priority areas, and outreach, collaboration, and dissemination efforts. The plan also emphasizes NIH’s commitment to research-sustaining activities and outlines future plans for tackling health disparities. |
___________________
11 See https://www.cdc.gov/healthequity/index.html (accessed April 29, 2024).
12 See https://www.nih.gov/about-nih/nih-wide-strategic-plan (accessed April 29, 2024).
13 See https://www.nimhd.nih.gov/docs/nimhd-strategic-plan-2021-2025.pdf (accessed April 29, 2024).
| Document Type | Agency | Report Title (Date) | Brief Summary of Document |
|---|---|---|---|
| Strategic Plan | NIH | EDI’s DEIA Strategic Plan (2023)14 | Developed by the NIH Office of Equity, Diversity, and Inclusion, this strategic plan responds to the executive order on DEIA in the federal workforce. It highlights NIH’s commitment to embracing and strengthening DEIA across its activities. It focuses on creating an inclusive environment that supports diversity and accessibility within the NIH workforce and its operations. |
NOTE: Although these reports may not specifically use the term “health equity,” they do address health care inequities and aim to promote equity in health outcomes.
issues of disparate treatment and discrimination within health care settings.15 Section 1557 of the ACA prohibits discrimination on the basis of race, color, national origin, age, disability, or sex (including sexual orientation and gender identity) from any health care provider (HCP) that receives federal funding. On April 26, 2024, OCR released a final rule that serves to clarify the standards that HHS applies in implementing Section 1557.16 OCR investigates complaints filed for noncompliant health programs, with penalties that could include suspending or losing federal funding. For example, OCR works toward accountability by providing guidance to states on their legal obligations to provide insurance coverage to children and families under the Children’s Health Insurance Program. This guidance has been critical during Medicaid unwinding after the Families First Coronavirus Response Act continuous enrollment condition expired.17
At a minimum, governmental and institutional efforts to overcome past and ongoing racism need to be able to identify a compelling need for race-conscious policies and pursue them only if they are narrowly tailored as the least restrictive means for furthering a compelling interest. These limits on remedies suggest the importance of broadening the focus to emphasize
___________________
14 See https://www.nih.gov/sites/default/files/about-nih/nih-wide-strategic-plan-deia-fy23-27.pdf (accessed April 29, 2024).
15 See https://www.hhs.gov/about/news/2024/04/01/ocr-health-equity-fact-sheet.html (accessed April 29, 2024).
16 See https://www.hhs.gov/civil-rights/for-individuals/section-1557/index.html (accessed April 29, 2024).
17 See https://www.hhs.gov/sites/default/files/medicaid-unwinding-letter.pdf (accessed April 28, 2023).
other factors linked to discrimination, such as low income, residential isolation, and underservice more generally.
Payment Policies
Health care provider (HCP) payment policies are integral to advancing health care equity (Bitton et al., 2019; Gold et al., 2021), but payment reform innovations have been evaluated against short-term savings rather than intentional choice to promote health care equity (NASEM, 2021). Therefore, the impact of these evolving models on health equity remains mixed when evaluated and more often unclear for policies that have not yet been well studied. As discussed in Chapter 4, given that payment-for-performance could exacerbate racial and ethnic health inequities, it is essential for these programs to be held accountable to provide equitable and quality care to minoritized populations (Conway and Satin, 2022; Weissman et al., 2012). In addition, adjusting for social risk factors in payment can help overcome the challenges and better match payments to address the care needs of minoritized populations.
HEALTH CARE DELIVERY SYSTEM
As discussed in Chapter 5, the health care workforce is not representative of the diverse U.S. population that is serves, and both federal and nonfederal partners can develop and support a diverse workforce essential for achieving equitable health care and optimal health for all. In addition, because accountability is necessary at the patient, HCP, payer, and health care system levels, each area requires exploration to ensure that appropriate accountability metrics and processes are being implemented. Many health care organizations have developed equity metrics to define and measure themselves, allowing for comparisons over time and with other organizations. Some have also appointed executive leaders to create and oversee health equity initiatives. Accrediting bodies for individual HCPs and large entities (e.g., hospitals, educational institutions, insurance companies) have also played a role. The next section presents an overview of accountability in the context of health care delivery systems.
Workforce Diversity
As discussed in Chapter 4, the ACA contained extensive authorized revisions to a wide range of health professions training programs. However, these amendments did not have mandatory funding. A lack of designated funding has hindered the vision of comprehensive change in how health professionals are defined, trained, and prepared to represent the health care
workforce—the backbone for delivering health services (see Chapter 5). Government and nongovernmental organizational actors can support the health care workforce in advancing health equity.
Government decision makers and agencies influence a range of structural levers that shape the federal, state, or local regulatory and fiscal context for the recruitment, training, and practice of health professionals and how much this context aligns with the health equity priorities outlined in this report. In particular, several promising structural-level strategies for improving workforce diversity and representativeness can be broadly categorized as representing fiscal support for programming that promotes recruiting and training underrepresented minority entrants for the health professions; the literature identifies regulatory facilitators (or barriers) for recruiting and training a diverse and representative body (Alegría et al., 2024; Rittenhouse et al., 2021). Affirmative action admissions policies are associated with an increase in underrepresented minority students in higher education, including in health professional education (Kelly-Blake et al., 2018; Long and Bateman et al., 2020; Ly et al., 2022). However, legislative and judicial challenges have arisen to institutional implementation of affirmative action. As discussed in Chapters 1 and 4, these developments could affect the training of health care professionals to meet the needs of the diverse U.S. population.
Federal, state, or local funding decisions about investments in different types of health care workforce development programs have implications for short- and long-term impacts on workforce diversity and representativeness (Rittenhouse et al., 2021). These include increasing residency or clinical training program capacity, establishing and strengthening loan repayment programs, providing service-contingent scholarship programs, and developing pathway programs designed to support high school, college, or post-baccalaureate students in acquiring the requisite experiences and skills for entry into health professional training.
Nongovernmental organizations also can support health care workforce alignment with health equity priorities at the structural level. Opportunities for building accountability through health education accreditation standards, health professional licensing and certification, and accreditation of health care organizations are promising.
Equity Metrics
Metrics that measure and track progress to advance racial and ethnic inequities have been created and adopted by health care systems, health insurance payers, professional organizations and accrediting bodies, and researchers. It is key to acknowledge that what is not measured cannot be effectively corrected, as accurate and comprehensive data are foundational
for addressing disparities (Penman-Aguilar et al., 2016). Tracking and documenting differences in health and health care–related outcomes between population groups is a common approach used by public health and health care delivery systems; however, measuring health equity is more complex and poses substantial challenges (Penman-Aguilar et al., 2016). Specifically, different definitions of health equity yield varying approaches to measurement, with some emphasizing fair opportunity for health and others focusing on eliminating disparities among marginalized groups compared to the majority (Braveman, 2017).
Several research studies and government and foundation reports have articulated methods for disparities measurement (Clemans-Cope et al., 2023; Dover and Belon, 2019; Duran et al., 2019; Penman-Aguilar et al., 2016). However, no agreed-upon standard exists for how health equity should be measured across individuals and populations in different health care contexts. Debate persists regarding the scope of health equity measures and whether they should be defined across social categories (e.g., race and ethnicity) or across individuals without regard to social categories. Frameworks for health equity measurement ranging from access to health care services to socioeconomic conditions within communities have emerged from these discussions (Ma et al., 2023; Sivashanker et al., 2020). Such frameworks aim to guide organizations in identifying measurable and actionable health inequities while also addressing the broader social determinants of health (SDOH).
One study that used several health equity metrics (including income disparities, Black–White disparities, health justice) to examine health equity progress over time found a lack of consistency across measures, however, it did clearly observe a lack of progress over the past 25 years (Zimmerman and Anderson, 2019). Another commonly used population-level health equity metric is the Social Vulnerability Index, which was developed by the Centers for Disease Control and Prevention and designed for public health emergencies and disasters. It allows for comparing the social vulnerability of one area to other areas through 16 census-level variables.18 Other metrics are used to measure health equity by focusing on community-level SDOH, including the Area Deprivation Index, county health rankings, child opportunity index, social deprivation index, and community resilience estimates index (Lines et al., 2023). The Centers for Medicare & Medicaid Services recently finalized health-equity-focused measures in care settings. This includes measures of hospital commitment to health equity and the percentage of adults screened for HRSNs.19 However, the lack of
___________________
18 See https://www.atsdr.cdc.gov/placeandhealth/svi/index.html (accessed April 29, 2024).
19 See https://www.cms.gov/files/document/health-equity-fact-sheet.pdf (accessed April 29, 2024).
agreed-upon standards for the appropriate use of these measures makes accountability through measurement and data tracking difficult. Also, Furthermore, screening for HRSNs without intervening to address these needs may sometimes more harmful than not screening (Butler et al., 2020).
Clinical Practice Guidelines (CPGs)
CPGs provide consistent standards for health professionals. Unfortunately, they are subject to the expertise of convened panels that often lack diversity and appropriate representation of racially and ethnically minoritized health professionals. The result is CPGs with vague and varied definitions of equity and inconsistently implemented accountability metrics (Boyles et al., 2023). A recent systematic review of U.S. pediatric-based CPGs found that many used race in potentially harmful ways that could lead to greater health inequities (e.g., suggesting that race was a risk factor for disease pathology) (Gilliam et al., 2022). Some CPGs are being updated to address equity issues, including accounting for the role of SDOH on health outcomes (Magnani and Brewer, 2022).
Variation in health care equity performance measures has posed significant challenges to accountability and advancing health care equity. In addition, different standards for acceptable performance measures to achieve optimal and equitable health for all have impeded efforts to hold health care systems, organizations, and providers accountable for their performance.
Chief Diversity and Equity Officers
The murders of George Floyd, Breonna Taylor, and Ahmaud Arbery in 2020 sparked public outrage on racism and once again forced many people to confront the role of structural racism in the nation’s criminal justice system (Nguyen et al., 2021). In addition, the COVID-19 pandemic highlighted longstanding racial and ethnic inequities in health and health care for minoritized communities (Ortega and Roby, 2021). Several professional organizations, including the American Medical Association and American Public Health Association, and a few federal agencies, including CDC, explicitly stated that racism negatively impacts the health of historically marginalized communities and is a fundamental driver of health inequities. Several cities, counties, and states made similar declarations (Mendez et al., 2021). This encouraged health care organizations to confront their shortcomings in diversity, equity (including health equity), and inclusion (DEI). As a result, health care organizations committed to addressing structural racism (Zephyrin et al., 2024). For some, this commitment included hiring Chief Diversity Officers (CDOs) and/or Chief Health Equity Officers (CHEOs).
The CDO role has become increasingly common within U.S. health care systems. It is not uniform, and the responsibilities vary. But, generally, many CDOs spearhead diversity initiatives to ensure culturally competent patient care and advance health equity in the broader community. Although internal-facing workforce diversity, equity, and inclusion efforts and external-facing health inequity reduction or elimination efforts may both require understanding structural and systemic racism, their goals and the training and skills necessary to successfully implement the respective programs are different. Health care organizations need to distinguish efforts aimed at workforce diversity from those targeting equity in patient care delivery and health in their catchment area (Crews et al., 2021).
No professional organization has conducted or commissioned an objective, neutral review on the role of CDOs in advancing racial and ethnic health care equity. However, a mixed-methods study on their role reported that many face obstacles in achieving health equity objectives within their hospitals and health care systems, including racist beliefs among staff, systemic and institutionally racist policies, lack of staff diversity, and lack of standardized metrics for measuring SDOH (Weissman et al., 2023). In some cases, health care systems are simultaneously appointing CDOs while also cutting funding for programs shown to advance health equity (e.g., primary care, mental health care). The emerging climate against diversity, equity, and inclusion in the form of legislative initiatives may negatively impact health equity efforts (Murray et al., 2023), including the sustainability of CDO and CHEO positions. However, data have not shown whether CDOs are being eliminated because of these efforts.
Licensing Bodies and Certification Boards
Licensing Bodies and Certification Boards for Individual Health Care Professionals
A large proportion of all health care professionals, and the vast majority of clinicians, are required to complete licensure examinations and maintain a professional certification to practice. Therefore, licensing bodies and certification boards set the standards for knowledge, skills, and continuing education expectations for large segments of the workforce and indirectly shape education, training, and continuing education offerings because schools and accreditation bodies are incentivized to increase alignment with the discipline-specific standards. However, incorporating critical health equity competencies in licensing exams and continuing education criteria for professional recertification remains an underused strategy to better prepare the workforce for equitable care delivery.
Additionally, licensing exams and continuing education are often unable to keep pace with the rapidly shifting knowledge base. For example, the U.S. Licensing Medical Examinations that all medical students and residents are required to pass have tasks/competencies that must be studied and learned (U.S. Medical Licensing Examination, 2024). None in the most recently published outline include health care equity principles, and one mention of cultural competence illustrates that this licensing body has not incorporate more accepted practices of cultural humility and structural competence (Frank and Shim, 2023).
Accrediting Bodies for Health Care Organizations
Accreditation of health care organizations by independent third parties represents a vital endorsement of quality and safety standards. As for health professional schools, accreditation criteria that embrace and promote interventions, care delivery models, and organizational practices and policies that improve health equity are powerful for incentivizing positive changes. Examples exist of increasing consideration of health equity in accreditation. For example, the Joint Commission includes requirements to reduce health disparities in its ambulatory health care, behavioral health care and human services, critical access hospitals, and hospital accreditation programs (Joint Commission, 2023a). Beginning in 2024, its National Patient Safety Goals include improving health equity, conceptualized as a health care quality issue, and identifying established leaders and standardized processes to measure health care disparities and integrate them into existing quality improvement plans (Joint Commission, 2023b). Similarly, the National Committee for Quality Assurance offers health care organizations opportunities for health equity accreditations (NCQA, 2024).
Specific programs for health equity accreditation also outline steps a hospital or other health care setting can take to identify and address equity gaps in access to high-quality care. Efforts to incorporate principles of health care equity into accreditation and certification processes have gained momentum. Health care equity has been recognized as a crucial aspect of care delivery, and many organizations are increasingly emphasizing the integration of equity principles into training and governance. Despite progress with accrediting bodies, more work remains. Greater accountability is needed to ensure that accreditation processes do not exacerbate inequities in health care.
Accrediting Bodies for Health Professional Schools.
The vast majority of U.S. health professional schools comply with accreditation criteria set by one or more discipline-specific professional organizations. These national criteria often represent influential roadmaps
for developing educational curricula and clinical or practical experiences. They shape practices and policies at institutions of health education. They are uniquely positioned to ensure that health equity-focused education and training is implemented across many sanctioned educational institutions. However, a review of accreditation criteria in the U.S and Canada found that essential competencies for equitable health care delivery were still omitted (Orban et al., 2022). Therefore, much of the positive potential of accrediting bodies for health professional education has not yet been fulfilled, and greater prioritization of health equity competencies is needed.
Accrediting Bodies for Insurance Companies.
Despite significant oversight and accountability for federal insurers, such as Medicaid and Medicare, private insurance companies have far less accountability. Most people are covered by private insurance, and the industry has significant power over clinical decision-making and contributes to barriers to timely access to health care (Pollack, 2023). No standardized or accepted accrediting bodies exist for private insurance companies, and efforts to increase oversight have not been successful. Private insurers create provider networks that are assessed by individual states for their “adequacy” or “inadequacy,” but accountability is limited for those that are considered inadequate. A Government Accountability Office survey of state oversight of provider plans found minimal accountability practices in place for private and employee-based provider networks (GAO, 2022).
COMMUNITY CENTEREDNESS AND ENGAGEMENT
As discussed in Chapter 4, a provision of the ACA helps to ensure the accountability of hospitals to promote health equity in the communities that they serve. Section 9007 requires that tax-exempt hospitals conduct community health needs assessments every 3 years, engaging the community in the process and developing a strategy for addressing identified needs.20 This statute is enforced by the Internal Revenue Service, which released final regulations in 2014 with guidance that requires input from “medically underserved, low-income, and minority communities” (Crossley et al., 2016). The Health Resources & Services Administration has similar (although not as extensive) regulations for needs assessments for federally qualified health centers.21
___________________
20 See https://www.irs.gov/charities-non-profits/community-health-needs-assessment-for-charitable-hospital-organizations-section-501r3 (accessed April 29, 2024).
21 See https://bphc.hrsa.gov/sites/default/files/bphc/compliance/hc-compliance-manual.pdf (accessed April 29, 2024).
Communities also can drive accountability toward health equity by ensuring that health systems incorporate community recommendations into their practices and policies. One example of this impact is the Pandemic and Racism Community Advisory Group, in which community-based organizations led by minoritized groups advised Public Health–Seattle & King County’s efforts on COVID-19 equity and antiracist interventions (Wysen et al., 2024). To ensure that the public health department effectively implemented the recommendations, the advisory group developed an accountability tool to ensure that decision makers were identified, actions taken, and outcomes measured. It saw 88 percent of its 75 recommendations partially or fully adopted by the health department (Wysen et al., 2024). It serves as a model for other community-based organizations to demand greater accountability in partnership with health care systems.
DATA AND RESEARCH INFRASTRUCTURE
As discussed in Chapter 7, data and research play a critical role in accountability, but challenges and limitations remain to building that infrastructure. Among the numerous examples of data shortcomings is the lack of health data granularization and access to the data for AIAN populations: despite strides in the last 20 years toward such granularization, access issues have limited the “practical and meaningful use for public health research” (Jamal et al., 2023).
Although the federal standardized classification categories for race and ethnicity categories can reveal many inequities, they also mask important health and health care inequities. Many individuals do not identify with the broad category options, resulting in potentially incomplete or inaccurate data (IOM, 2009; NASEM, 2023; Pellegrin et al., 2016). In 2022, OMB convened the Federal Interagency Technical Working Group on Race and Ethnicity Standards, with statistical agencies and other federal agencies to review the standard. In March 2024, OMB released revised race and ethnicity data standards that add Middle Eastern or North African as a new minimum category and require collecting more detailed race, ethnicity, and tribal affiliation beyond the minimum categories as the default. Federal agencies are expected to submit an Agency Action Plan for complete compliance with the updated standards within 18 months and to be fully compliant within 5 years.22 OMB plans to establish an Interagency Committee on Race and Ethnicity Statistical Standards that will “maintain and carry
___________________
22 See https://www.federalregister.gov/documents/2024/03/29/2024-06469/revisions-to-ombs-statistical-policy-directive-no-15-standards-for-maintaining-collecting-and (accessed April 1, 2024).
out a government-wide research agenda and undertake regular reviews of the standards.”23
Neither the current nor the newly revised OMB directive on race and ethnicity standards requires federal agencies to collect these data but rather specify minimum reporting categories for those agencies that do so. Additionally, although proposed updates require collecting detailed race, ethnicity, and tribal affiliation categories as the default, the standard does not stipulate how to report such data. Researchers, health care professionals, and policy makers have stressed the need to both collect and report disaggregated racial, ethnic, and tribal data. OMB provides guidelines on how these more granular data should be handled, but these are subjective and often do not reflect individual self-identities (Holup et al., 2007).
CHAPTER SUMMARY
Greater accountability is necessary to ensure that progress is made in achieving equitable outcomes in health care. Accountability is fundamentally a leadership function. It starts with policy makers, health care leaders, and HCPs at all levels having the core value that achieving optimal health for all people is important and then putting that belief into action. It means they have to have a sound understanding of the interrelationships between health outcomes and the systems that empower or undermine them. To improve accountability processes, clear goals and objectives need to be identified, metrics standardized to ensure tracking progress toward goals, and consequences imposed for those that do not achieve these goals and objectives (Frank and Shim, 2023). First, to improve accountability, standards for accreditation for health professions, schools should be updated to include the best available science related to competencies for health equity. This can be expanded to continuing education and professional licensing bodies. Increased standards will help to ensure a more diverse workforce with greater knowledge and expertise on principles of health equity. Regarding clinical care, performance metrics need to be more inclusive and reliant on patient experiences; typically, patient satisfaction is an afterthought for many performance metrics, especially mental health and SUD treatment (Frank and Shim, 2023).
Second, incentives in the health care system need to be aligned with the goals. A major barrier to greater accountability in health care equity is a system designed to rely on market forces, when equitable outcomes are often not based on capitalist structures (Frank and Shim, 2023). Efforts to address this challenge have been based on pay-for-performance metrics,
___________________
23 See https://www.federalregister.gov/documents/2024/03/29/2024-06469/revisions-to-ombs-statistical-policy-directive-no-15-standards-for-maintaining-collecting-and (accessed April 1, 2024).
which have demonstrated issues in promoting equitable outcomes, as providers can “cherry-pick” and refuse to care for more complex patients, including those with LEP (Frank and Shim, 2023).
Third, greater standardization of data and metrics that track equity is also a key component of improved accountability. Robust data collection, tracking, and reporting efforts built on uniform standards can help to increase consistency toward equity goals.
Finally, increased accountability in the legal and policy arena is critical. National goals, objectives, and standards for equity are needed, but the landscape has many different federal agencies and private and public sector organizations all working independently to achieve equity goals. Identifying a national standard that is coupled with metrics that could be tracked to ensure progress is made and adequate resources are devoted to achieving the goals could drive greater accountability. Many of the individual federal reports and plans are valuable, but a specific national plan (similar to Healthy People24, for example) would prevent a diffusion of efforts and allow limited resources to be used more effectively and efficiently.
Based on the materials in this chapter, the committee offers these conclusions:
Conclusion 8.1. Several HHS and other federal agencies have strategic plans, frameworks, or policy statements that aim to address health care inequities and advance health equity. These plans, frameworks, and policy statements are often disparate and siloed and do not represent coordinated efforts.
Conclusion 8.2. There is no widely agreed-upon systematic standards and procedures for acceptable performance measures to achieve equitable health care and optimal health for all irrespective of race and ethnicity and socioeconomic background.
Conclusion 8.3. No federal oversight body or professional organization has conducted or commissioned an evaluation of all the goals proposed or programs implemented by the health care equity-related strategic plans and other policy frameworks across the federal government.
Conclusion 8.4. Some clinical practice guidelines used to provide consistent standards for health care professionals are subject to the expertise of convened panels who often lack diversity and representation of racial and ethnically minoritized health professionals.
Conclusion 8.5. Most health care payment models do not explicitly tie payment to reducing racial and ethnic health care inequities advancing health equity.
___________________
24 See https://health.gov/healthypeople (accessed April 24, 2024).
REFERENCES
Alegría, M., I. B. Thurston, M. Cheng, C. Herrera, S. L. Markle, I. S. O’Malley, D. Porter, R. Estrada, and N. Giraldo-Santiago. 2024. A learning assessment to increase diversity in academic health sciences. Journal of the American Medical Association Health Forum 5(2).
Blumenthal, D., C. Lewis, and M. K. Abrams. 2021. Making health care accountable considerations for the Center for Medicare and Medicaid Innovation. The Commonwealth Fund. https://www.commonwealthfund.org/blog/2021/making-health-care-accountable (accessed April 29, 2024).
Bitton, A., J. Fifield, H. Ratcliffe, A. Karlage, H. Wang, J. H. Veillard, D. Schwarz, and L. R. Hirschhorn. 2019. Primary healthcare system performance in low-income and middle-income countries: A scoping review of the evidence from 2010 to 2017. BMJ Global Health 4(Suppl 8):001551.
Boyles, C. M., P. Spoel, P. Montgomery, M. Nonoyama, and K. Montgomery. 2023. Representations of clinical practice guidelines and health equity in healthcare literature: An integrative review. Journal of Nursing Scholarship 55(2):506-520.
Braveman, P. 2017. A new definition of health equity to guide future efforts and measure progress. Health Affairs Forefront.
Butler, E. D., A. U. Morgan, and S. Kangovi. 2020. Screening for unmet social needs: Patient engagement or alienation? New England Journal of Medicine Catalyst Innovations in Care Delivery 1(4).
Clemans-Cope, L., B. Garrett, and S. McMorrow. 2023. How should we measure and interpret racial and ethnic disparities in health care? https://www.urban.org/research/publication/how-should-we-measure-and-interpret-racial-and-ethnic-disparities-health-care (accessed April 29, 2024).
Conway, A., and D. Satin. 2022. The role of pay-for-performance in reducing healthcare disparities: A narrative literature review. Preventive Medicine 164:107274.
Crews, D. C., C. A. Collins, and L. A. Cooper. 2021. Distinguishing workforce diversity from health equity efforts in medicine. Journal of the American Medical Association Health Forum 2(12):e214820.
Crossley, M., E. T. Tyler, and J. L. Herbst. 2016. Tax-exempt hospitals and community health under the Affordable Care Act: Identifying and addressing unmet legal needs as social determinants of health. Public Health Reports 131(1):195-199.
Dover, D. C., and A. P. Belon. 2019. The health equity measurement framework: A comprehensive model to measure social inequities in health. International Journal for Equity in Health 18(1):1-12.
Duran, D., Y. Asada, J. Millum, and M. Gezmu. 2019. Harmonizing health disparities measurement. American Journal of Public Health 109(S1):S25-S27.
Frank, R. G., and R. S. Shim. 2023. Toward greater accountability in mental health care. Psychiatric Services 74(2):182-187.
GAO (Government Accountability Office). 2022. Private health insurance: State and federal oversight of provider networks varies. GAO-23-105642. Washington, DC: Government Accountability Office.
Gilliam, C. A., E. G. Lindo, S. Cannon, L. Kennedy, T. E. Jewell, and J. S. Tieder. 2022. Use of race in pediatric clinical practice guidelines: A systematic review. Journal of the American Medical Association Pediatrics 176(8):804-810.
Gold, S. B., L. A. Green, and J. M. Westfall. 2021. Heeding the call for urgent primary care payment reform: What do we know about how to get started? The Journal of the American Board of Family Medicine 34(2):424-429.
Holup, J. L., N. Press, W. M. Vollmer, E. L. Harris, T. M. Vogt, and C. Chen. 2007. Performance of the U.S. Office of Management and Budget’s revised race and ethnicity categories in Asian populations. International Journal of Intercultural Relations 31(5):561-573.
IOM (Institute of Medicine). 2009. Race, ethnicity, and language data: Standardization for health care quality improvement. Washington, DC: National Academies Press.
Jamal, A., M. Srinivasan, G. Kim, R. J. Huang, and L. Palaniappan. 2023. Why are we going backward? Barriers to disaggregated racial information in Federal data sets. American Journal of Public Health 113(8):852-855.
The Joint Commission. 2023a. New requirements to reduce health care disparities. https://www.jointcommission.org/standards/r3-report/r3-report-issue-36-new-requirements-to-reduce-health-care-disparities/ (accessed April 29, 2024).
The Joint Commission. 2023b. National Patient Safety Goals® effective January 2024 for the hospital program. https://www.jointcommission.org//media/tjc/documents/standards/national-patient-safety goals/2024/npsg_chapter_hap_jan2024.pdf (accessed April 29, 2024).
Kelly‐Blake, K., N. A. Garrison, F. E. Fletcher, B. Ajegba, N. Smith, M. Brafford, and E. Bogdan‐Lovis. 2018. Rationales for expanding minority physician representation in the workforce: A scoping review. Medical Education 52(9):925-935.
Lines, L. M., M. C. Long, S. Zangeneh, K. DePriest, J. Piontak, J. Humphrey, and S. Subramanian. 2023. Composite indices of social determinants of health: Overview, measurement gaps, and research priorities for health equity. Population Health Management 26(5):332-340.
Long, M. C., and N. A. Bateman. 2020. Long-run changes in underrepresentation after affirmative action bans in public universities. Educational Evaluation and Policy Analysis 42(2):188-207.
Ly, D. P., U. R. Essien, A. R. Olenski, and A. B. Jena. 2022. Affirmative action bans and enrollment of students from underrepresented racial and ethnic groups in us public medical schools. Annals of Internal Medicine 175(6):873-878.
Ma, S., S. Agrawal, and R. Salhi. 2023. Distinguishing health equity and health care equity: A framework for measurement. NEJM Catalyst Innovations in Care Delivery 4(2).
Magnani, J. W., and L. C. Brewer. 2022. Leaving the social vacuum: Expanding cardiovascular guidelines to embrace equity. Circulation 146(3):156-158.
Mendez, D. D., J. Scott, L. Adodoadji, C. Toval, M. McNeil, and M. Sindhu. 2021. Racism as public health crisis: Assessment and review of municipal declarations and resolutions across the United States. Frontiers in Public Health 9:686807.
Murray, T. A., S. Oerther, and K. J. Simmons. 2023. Anti-DEI legislation targeting colleges and universities: Its potential impacts on nursing education and the pursuit of health equity. Nursing Outlook 71(4):101994.
NASEM (National Academies of Sciences, Engineering, and Medicine). 2021. Implementing high-quality primary care: Rebuilding the foundation of health care. Washington, DC: The National Academies Press.
NASEM. 2023. Federal policy to advance racial, ethnic, and tribal health equity. Washington, DC: The National Academies Press.
NCQA (National Committee for Quality Assurance). 2024. NCQA’s health equity accreditation programs. https://www.ncqa.org/programs/health-equity-accreditation/ (accessed April 29, 2024).
Nguyen, T. T., S. Criss, E. K. Michaels, R. I. Cross, J. S. Michaels, P. Dwivedi, D. Huang, E. Hsu, K. Mukhija, and L. H. Nguyen. 2021. Progress and push-back: How the killings of Ahmaud Arbery, Breonna Taylor, and George Floyd impacted public discourse on race and racism on Twitter. SSM-Population Health 15:100922.
Orban, J., C. Xue, S. Raichur, M. Misak, A. Nobles, J. Casimir, and S. Batra. 2022. The scope of social mission content in health professions education accreditation standards. Academic Medicine 97(1):111-120.
Ortega, A. N., and D. H. Roby. 2021. Ending structural racism in the US health care system to eliminate health care inequities. Journal of the American Medical Association 326(7):613-615.
Rittenhouse, D., A. Ament, J. Genevro, and K. Contreary. 2021. Health workforce strategies for California: A review of the evidence. Mathematica Policy Research Reports.
Pellegrin, K. L., J. B. Miyamura, C. Ma, and R. Taniguchi. 2016. Improving accuracy and relevance of race/ethnicity data: Results of a statewide collaboration in Hawaii. Journal for Healthcare Quality 38(5):314-321.
Penman-Aguilar, A., M. Talih, D. Huang, R. Moonesinghe, K. Bouye, and G. Beckles. 2016. Measurement of health disparities, health inequities, and social determinants of health to support the advancement of health equity. Journal of Public Health Management & Practice 22(Suppl 1):S33–42.
Pollack, R. 2023. Health insurance barriers delay, disrupt and deny patient care. U.S. News.
Sivashanker, K., T. Duong, A. Resnick, and S. Eappen. 2020. Health care equity: From fragmentation to transformation. NEJM Catalyst Innovations in Care Delivery 1(5).
Weissman, J. S., R. Hasnain-Wynia, R. M. Weinick, R. Kang, C. Vogeli, L. Iezzoni, and M. B. Landrum. 2012. Pay-for-performance programs to reduce racial/ethnic disparities: What might different designs achieve? Journal of Health Care for the Poor and Underserved 23(1):144–160.
Weissman, J. S., R. R. Adler, J. Betancourt, A. Tan-McGrory, J. A. Lewis, C. M. DesRoches, A. Pomer, E. Singh, A. Liebig, and S. Ilkhani. 2023. How hospitals are addressing the effects of racism: A mixed-methods study of hospital equity officers. Health Affairs 42(10):1402–1410.
Wysen, K., M. Valenzuela, W. E. Barrington, Y. Teferi, A. Evans, B. Kiros, M. Merriweather, and M. Zuniga. 2024. Public health accountability in action: The King County pandemic and racism community advisory group. Public Health Reports:00333549231223923.
Zephyrin, L., M. Ayo-Vaughan, A. Bossick, A. Noroña-Zhou, E. Higginbotham, M. Richardson, H. Rodriguez, and A. Bryant. 2024. Stakeholders’ viewpoints on working to advance health equity. Health Equity 8(1):14–25.
Zimmerman, F. J., and N. W. Anderson. 2019. Trends in health equity in the United States by race/ethnicity, sex, and income, 1993–2017. Journal of the American Medical Association Network Open 2(6):e196386-e196386.
This page intentionally left blank.

























