Learning What Works: Infrastructure Required for Comparative Effectiveness Research: Workshop Summary (2011)
Chapter: Appendix D: Comparative Effectiveness Research Priorities: FCCCER Recommendations (2009)
Appendix D
Comparative Effectiveness
Research Priorities:
FCCCER Recommendations (2009)
PRIORITY RECOMMENDATIONS FOR OFFICE OF SECRETARY CER FUNDS1
Using the strategic framework for CER discussed in Section V, and taking into consideration the unique role that OS funds can play in addressing high priority gaps, the Council developed a recommended high-level investment strategy for the use of the OS ARRA funds. The strategy has three different levels of priority recommendations for OS fund investments in the Core Activities and Cross-cutting Priority Themes in the CER framework (Figure 3).
- Primary investment. This area of investment should represent a large portion of the OS funds. It best fulfills the full range of prioritization criteria and requires scaled investment in order to be successful. The Council recommends that CER Data Infrastructure be the primary investment.
- Secondary investments. These areas should also receive significant investment. They are as critical to success in CER as the primary focus, but individually may require a smaller amount of funding to be successful. The Council recommends that Dissemination and
_________________
1 Passage from the Federal Coordinating Council for Comparative Effectiveness Research Report to the President and Congress, June 30, 2009. Department of Health and Human Services.
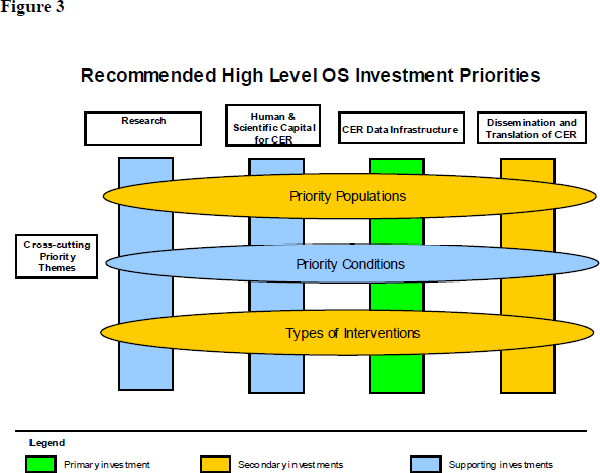
Translation of CER, Priority Populations, and Priority Types of Intervention be secondary investments.
- Supporting investments. These areas should not be the major focus of OS funding as they do not fulfill the prioritization criteria as well as primary and secondary investments, but some funding may be necessary to support and enable investments in higher priority areas and fill identified gaps. The Council recommends that Human and Scientific Capital, Research, and Conditions receive supporting investments. It is important to note that these recommendations pertain only to OS funds; AHRQ, NIH, and VA have a history of significant investments in Research, Human and Scientific Capital, and Conditions.
The Council believes that this strategy and distribution of investments will best position the Secretary to:
- Respond to patient and physician demand for CER.
- Balance achieving near-term results with building longer-term opportunities.
- Capture the distinctive value of the Secretary’s ARRA funds.
While it is the responsibility of the Office of the Secretary to operationalize this strategy, the Council’s rationale for these recommendations is designed to help guide the Secretary in making specific investment decisions. The Council based its rationale for each level of investment in the strategy on the prioritization criteria described above, as well as representative examples of investment in each area proposed through the public comment process and by federal agencies.
Primary Investment
CER data infrastructure development is the most distinctive opportunity for OS ARRA funding. It requires a large, up-front infusion of capital to be successful that is unlikely to come from any source other than OS ARRA funds, making it ideal for this funding mechanism. It has broad potential impact, with the ability for resulting research to address conditions and populations captured in the primary data. Given the absence of comprehensive databases and data evaluation tools, there is significant demand from the patient, clinical, and public health communities for new, expanded data infrastructure and data access to support decision making. Finally, investments in data infrastructure have the potential to generate significant additional investments in two ways. First, some of these investments could take the form of public-private partnerships. Second, data infrastructure is a tool that, once developed, will result in new research conducted and/or funded by entities such as biomedical research organizations, payers, foundations, and health care providers.
The Council received proposals on a number of potentially promising initiatives related to data infrastructure, including but not limited to:
- Building, expanding, and linking longitudinal administrative claims databases.
- Linking administrative data with EHR-based or registry data.
- Expanding high-impact patient registries (e.g., collaborations with specialty organizations, SEER).
- Distributed data networks populated by EHRs in practice and provider settings.
- Expanding analysis of FDA and private sector data on drug and device trials and safety.
As the Office of the Secretary identifies specific opportunities in data infrastructure, the Council recommends that it consider most carefully those that:
- Expand access to existing resources, especially those currently managed by Federal agencies.
- Create scaled platforms by leveraging existing data and capabilities in the private sector.
- Capitalize on linkages between health IT investments and the potential for CERinfrastructure to develop evidence to inform decision making.
- Ensure that infrastructure is responsive to needs of patients, providers, and other decision makers—and not driven by what is most feasible.
The Council appreciates the relationship and need for coordination between CER and health IT (e.g., through a distributed network of EHRs) investments. As the Secretary develops HHS’s full portfolio of ARRA investments, it will be critical to consider both CER and health IT holistically, not as policy silos, recognizing that success in CER is largely dependent on success in health IT and vice versa. With all data infrastructure investments, the government will need to ensure data security and privacy. Protecting security and privacy is key to maintaining the public’s trust.
Secondary Investments
Secondary investments include a core area of investment—Dissemination and Translation of CER—and two cross-cutting themes—Priority Populations and Types of Intervention.
Dissemination, translation and adoption of CER is about realizing the benefits that comparative effectiveness research has to offer both patients and providers. While the breadth and depth of the near-term impact depends on what types of pilot programs the OS supports, the lessons and tools for translation developed by those pilots will be relevant to all.
The lack of reliable success in disseminating findings from CER in ways that translate into better health outcomes highlights the uncertainty and difficulty of this enterprise. However, dissemination and translation is essential to improving outcomes for patients and the link between evidence production and how best to get this information to physicians and patients in a way they understand is critical to capitalizing on the CER investment. Despite important efforts by the federal government, especially AHRQ, NIH, VA and DoD, the majority of current funding goes to building evidence as opposed to ensuring that the existing evidence base is utilized in
patient care and health systems management. This creates a unique role for OS ARRA funding. Investments in dissemination and translation programs also have the potential to generate additional investments, especially from providers, if private institutions elect to implement similar efforts or partner with the Federal Government on translation efforts.
There are a wide range of potential dissemination, translation and adoption programs that the OS could support, including:
- Investing in dissemination and translation of CER findings throughout the Federal delivery system.
- Dissemination and translation through partnerships with provider and/or patient organizations.
- Decision support and shared decision-making tools to provide information to clinicians and patients at the point of care.
- Developing standards for communication tools for patients and providers, (e.g., a patient-friendly simple scoring system).
- Partnering with an existing consumer media channel (e.g., Internet search engine or health information site) to expand patient access to existing CER data.
- Creating a National Patient Library with a primary focus on providing evidence to patients in easy-to-use and understandable formats.
The Council recommends that the Office of the Secretary consider the following in making investments in dissemination and translation:
- Investing in better understanding the most effective methods to disseminate and translate research findings to improve patient outcomes.
- Identifying opportunities both to develop tools for translation and to pilot implementation of these tools.
- Partnering with provider organizations in federal agencies, as well as in states and the private sector.
- Accounting for potential surrogate decision makers (e.g., families) and the context for decisions in patient-focused tools.
- Ensuring that programs address a specific need articulated by the implementing organization or the partner to ensure success and the sustainability ofdissemination activities.
- Focusing on developing standards for communication.
- Increasing understanding of the most effective methods to disseminate findings to clinicians and patients to inform decision making.
From an operational perspective, investments in the cross-cutting themes are somewhat distinct from investments in the core areas. Whereas funding for a core area might go to a project or organization focused on a specific activity, funding for a cross-cutting theme requires multiple coordinated investments and activities to be successful. Investments in these themes could cover some or all of the four core activities: research, data infrastructure, human and scientific capital, and dissemination and translation. These investments could involve a coordinated investment across HHS or the federal government, or they could be focused in academic centers, integrated delivery system organizations, private industry, or other nongovernmental entities. Collaborative efforts to inform and transform care will be essential to achieving meaningful impact across these cross-cutting themes.
Investments in specific populations, meanwhile, will help ensure that the benefits of CER are available to all. It can also focus CER efforts on populations with existing health disparities and worse outcomes. CER has the potential in some populations, such as racial and ethnic minorities, to fill critical gaps that, historically, efficacy research has left unaddressed.
The Council identified several populations for whom the Secretary should consider allocating CER funds:
- Racial and ethnic minorities
- Persons with disabilities
- Elderly
- Children
- Patients with multiple chronic conditions
Investment in specific types of interventions in a cross-cutting manner also presents a unique opportunity for the nation’s health system. The Council has identified six specific interventions for the Secretary to consider that address large and varied populations, resulting in high potential impact, are areas of high clinical uncertainty, and are not being adequately addressed by other entities. They are:
- Medical and assistive devices (e.g., comparing rehabilitative devices).
- Procedures and surgery (e.g., evaluating surgical options or surgery versus medical management).
- Diagnostic testing (e.g., comparing imaging modalities for evaluating certain types of cancer).
- Behavioral change (e.g., developing and assessing smoking cessation programs).
- Delivery system strategies (e.g., testing two different discharge process care models on readmission rates or testing two different medical home models on preventing hospital admissions and improving quality of life).
- Prevention (e.g., comparing two interventions to prevent or decrease obesity, comparing strategies for reaching populations that do not access the healthcare system with prevention efforts).
Furthermore, the Council recommends that the Office of the Secretary consider the following in making investments in the cross-cutting themes of priority populations and types of interventions:
- Focusing on immediate, specific patient needs that can generate results.
- Concentrating on areas with cross-cutting gaps in research, data infrastructure, scientific capital, and/or translation.
- Building on promising systems and practices already in place, both within the government and in the private sector, and measuring results when scaled up and disseminated.
- Strongly encouraging coordination across the government and with entities outside of the government.
Supporting Investments
The Council recommends that the OS reserve some ARRA funding for Research, Human & Scientific Capital, and the Conditions cross-cutting theme. Because these investments and topics are the major foci of CER activities at NIH and AHRQ, both of which will likely utilize ARRA funds administered by those organizations for these purposes, they do not represent distinctive investment for OS funds. However, there will likely be targeted investments in these areas that could support other OS ARRA efforts, such as training new researchers in CER methods or addressing gaps not addressed elsewhere in the federal government.
In making these targeted investments, the Council recommends the Office of the Secretary consider:
- Focusing on areas that maximize the value of the Secretary’s investments in other areas.
- Avoiding duplication of efforts with other agencies.
For all of the above investments, the Council recommends that the Office of the Secretary consider the portfolio of investments and where synergies exist to leverage one investment into multiple areas. For example,
a data infrastructure investment that can also be used for a cross-cutting priority theme would be of higher value than an investment that has more limited applications. Doing so will help to ensure that the funds allocated to the Office of the Secretary for CER will have a significant positive impact on the quality of patient care in the near term, and lay the foundations for continued improvements going forward.







